Study Estimates How Common Orthostatic Intolerance, POTS, and Low Blood Pressure Are in Long COVID
Title: The prevalence of orthostatic intolerance, postural orthostatic tachycardia syndrome and orthostatic hypotension in post-acute sequelae of COVID-19.
Plain-Language Summary
This paper asks a straightforward epidemiology question: among people with post-acute sequelae of COVID-19 (PASC, often called Long COVID), how common are forms of autonomic dysfunction that cause symptoms when standing? The autonomic nervous system controls “automatic” body functions such as heart rate and blood pressure. When it malfunctions, people can develop symptoms triggered by upright posture (orthostatic intolerance).
The authors performed a systematic review and meta-analysis following PRISMA 2020 guidelines. They searched multiple databases (including PubMed, Embase, and CENTRAL) for studies up to February 1, 2025, and included 21 observational studies that reported prevalence of orthostatic intolerance (OI), postural orthostatic tachycardia syndrome (POTS), and/or orthostatic hypotension (OH) in PASC. In total, the pooled dataset included 2,916 participants, with a high proportion of women and post-COVID symptom durations ranging roughly from 12 to 72 weeks.
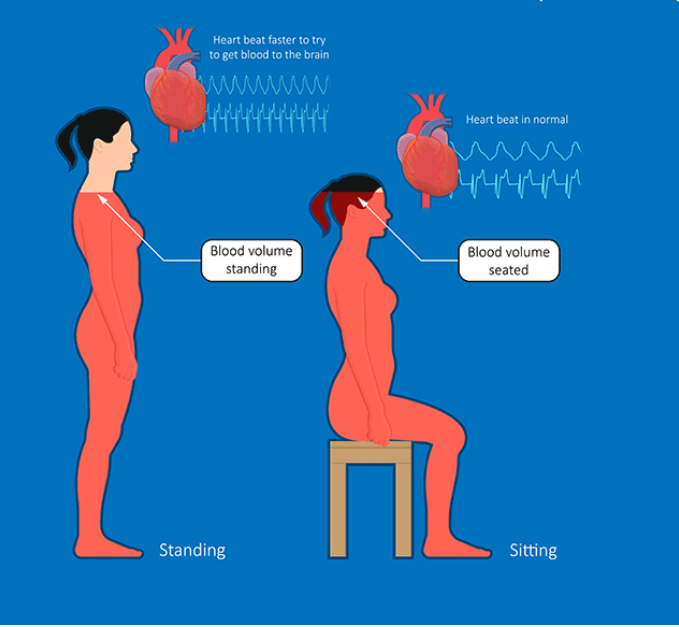
For definitions: orthostatic intolerance (OI) is an umbrella term for symptoms provoked by standing and relieved by lying down. POTS is diagnosed when heart rate rises substantially after standing (typically within 10 minutes) without meeting criteria for classic orthostatic hypotension; OH is diagnosed when blood pressure drops significantly shortly after standing or during a tilt-table test. Many included studies used objective tests such as head-up tilt (HUT) or active standing tests; some used symptom questionnaires (e.g., COMPASS-31) for OI.
Using random-effects models (chosen because the included studies differed in design, populations, and testing protocols), the authors estimated pooled prevalences of 70.6% for OI, 36.2% for POTS, and 18.6% for OH among people with PASC. However, the POTS and OH estimates showed substantial between-study heterogeneity (i.e., results varied widely across studies), and the certainty of evidence (GRADE) was rated low for OI and OH and very low for POTS.
The team also explored factors that might explain differences between studies. Meta-regression suggested that higher average age was associated with lower reported prevalence of POTS and OH. Subgroup analyses suggested higher POTS and OH prevalence in cohorts described as having mild (versus moderate/severe) acute COVID-19, though these comparisons are limited by the composition and reporting of the available studies. Publication bias signals were minimal for OH but were suggested for POTS, and an adjustment method (trim-and-fill) substantially reduced the POTS pooled estimate—highlighting uncertainty in the true population prevalence.
Key Findings
- Pooled prevalence estimates in PASC: orthostatic intolerance (OI) 70.6% (95% CI 66.8%–74.5%), POTS 36.2% (95% CI 18.6%–53.8%), and orthostatic hypotension (OH) 18.6% (95% CI 8.6%–28.7%).
- Heterogeneity was high for POTS and OH (study-to-study results varied widely), indicating that prevalence depends strongly on cohort selection, diagnostic methods, and study context.
- Age association: meta-regression found a significant negative association between advancing age and reported prevalence of POTS and OH across studies.
- Severity subgroup signal: subgroup analyses suggested higher POTS and OH prevalence in cohorts with mild acute COVID-19 compared with moderate/severe, though data for moderate/severe were limited.
- Publication bias and uncertainty (POTS): bias assessments suggested possible publication bias for POTS; trim-and-fill adjustment reduced the pooled POTS estimate substantially, reinforcing uncertainty.
- Evidence certainty (GRADE): low certainty for OI and OH estimates and very low certainty for POTS, driven by inconsistency, risk of bias, and possible publication bias.
Study Type
This is a systematic review and meta-analysis (observational prevalence synthesis) following PRISMA 2020 guidelines, based on 21 observational studies.
What This Means (and Doesn’t Mean)
Scientifically, these results suggest that orthostatic symptoms and measurable autonomic abnormalities are commonly reported among people studied with PASC, and that prevalence estimates can be high—especially for orthostatic intolerance as a broad syndrome. The analysis also supports the idea that cohort characteristics (such as age distribution) and measurement protocols (questionnaire-based screening versus objective tilt/standing tests) meaningfully influence reported rates, which matters for interpreting and comparing studies.
At the same time, the meta-analysis does not establish a single “true” global prevalence for POTS or OH in all Long COVID populations because the underlying studies are heterogeneous and often drawn from specialized clinical settings. The findings do not prove causality (i.e., they do not demonstrate that SARS-CoV-2 directly causes these autonomic conditions in any individual), and they do not determine mechanisms. The results also do not provide validated clinical screening or treatment recommendations; they primarily quantify what has been reported in the existing literature and highlight uncertainty where evidence quality is limited.
Source
Disclaimer
This summary was created with the assistance of artificial intelligence and reviewed by a human prior to publication. While care is taken to ensure accuracy, errors are possible. If you notice any issues, have questions, or would like to request coverage of a specific research paper, please contact admin@long-covid.org.
Share
If you found this summary helpful, please consider sharing it. It helps more people find clear, trustworthy Long COVID research.
Share on X Share on Facebook Share on Threads Copy link for Instagram




